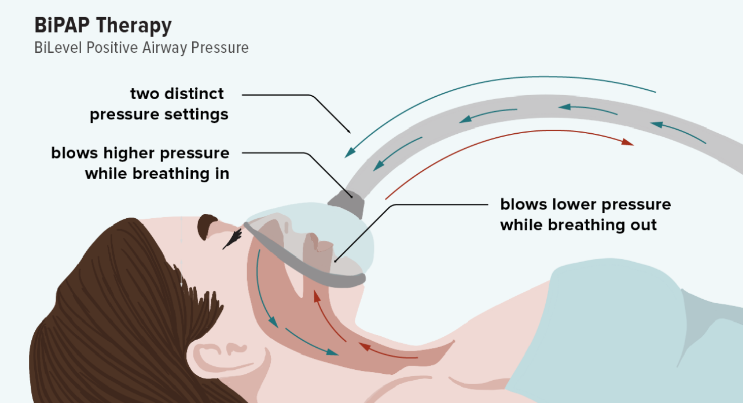
Amyotrophic Lateral Sclerosis (ALS) is a progressive disease with degeneration of motor neurons in the brain and spinal cord causing weakness, muscle atrophy, fasciculations and spasticity. The etiology of ALS is not fully understood, likely resulting from a complex interplay between genetics and environmental factors. ALS can affect the respiratory muscles used to breathe. The nerves that control the breathing muscles do not work correctly, and the muscles become weak. Although this usually occurs in late stages of the disease, in some cases it can occur in the early stages. Weak breathing muscles can make it challenging to take a deep breath. Patients with ALS start to breathe shallowly as a result which affects their ability to effectively exchange air in the lungs. Non-invasive ventilation (NIV) is recommended for people diagnosed with ALS who meet specific criteria per the Canadian Best Practice Guidelines for ALS Management. NIV is a machine that supports a persons breathing using either nasal or full face mask. Generally patients with ALS are prescribed a Bi-level positive airway pressure (BiPAP), which is a type of NIV, that delivers two pressure levels: a higher pressure when a person inhales and a lower pressure when a person exhales. The BiPAP compensates for diaphragm weakness and helps improve overall quality of life for those living with ALS. A person is generally assessed every three months by a respirologist who determines if NIV is an appropriate treatment option. Timely testing is important for people diagnosed with ALS as their respiratory status can change quickly. This includes overnight oximetry which may be ordered by a respirologist to determine if NIV is to be considered. Oxygen should not be considered a routine treatment for chronic respiratory insufficiency. In patients with ALS with acute hypoxemia, management of respiratory insufficiency with NIV needs to be considered first. If hypoxemia remains after optimal NIV pressure is applied, the etiology of the hypoxia needs to be assessed and supplemental oxygen can be considered. If a respirologist determines that oxygen therapy should be utilized, it is recommended to utilize oxygen therapy together with BiPAP to ensure they are able to effectively breath out carbon dioxide and avoid hypoxemia. Kala Bolt (she/her), RN BSN, CNNClinical Nurse Coordinator – ALS/MND Clinic
Saskatoon City Hospital - Saskatoon References: Canadian best practice recommendations for the management of amyotrophic lateral sclerosis - CMAJ 2020 November 16;192:E1453-68. doi: 10.1503/cmaj.191721 ALS Guide – ALS Society https://www.als.ca/wp-content/uploads/2020/03/ALS-guide-ON-EN-WEB.pdf |